Motiva Breast Implants Over the Muscle: 2026 Pros & Cons

TL;DR
Motiva breast implants over the muscle refers to placing the implant above the pectoral muscle rather than beneath it. This approach has historically carried higher risks of capsular contracture and visible rippling, but Motiva’s SmoothSilk surface and Ergonomix gel technology have changed that equation. Surgeons with decades of experience are now reconsidering over-the-muscle placement because Motiva’s clinical data shows capsular contracture rates as low as 0.5% at five years, regardless of placement plane. For the right candidate, this means faster recovery, no animation deformity, and a natural look that older implant generations couldn’t reliably deliver in this position.
What “Over the Muscle” Actually Means
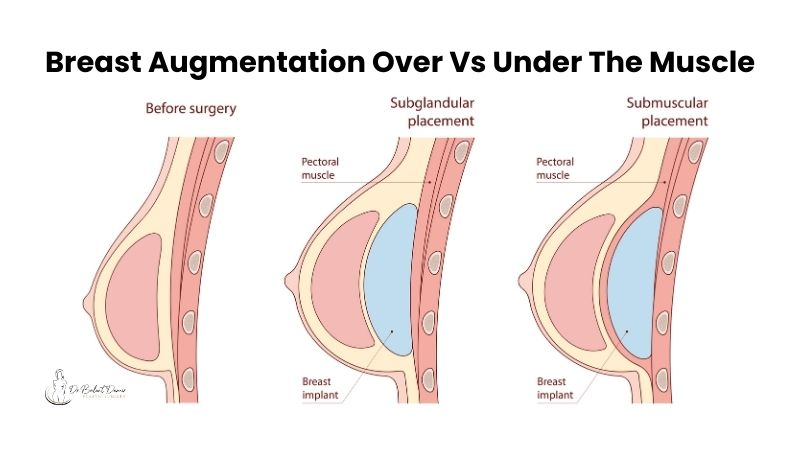
When someone says “Motiva breast implants over the muscle,” they’re describing a breast augmentation where the implant sits above the pectoralis major muscle instead of beneath it. The implant rests directly under the breast tissue (or under a thin tissue layer called fascia), rather than being tucked behind the chest muscle.
This placement goes by several clinical names: subglandular, subfascial, or prepectoral. All three fall under the “over the muscle” umbrella, though they differ in subtle but meaningful ways.
The opposite approach, submuscular or dual plane placement, tucks the implant partially or fully under the pectoralis muscle. For over 30 years, submuscular placement was the default in the United States and Canada because older implants placed above the muscle had higher rates of capsular contracture and visible rippling. Motiva’s technology is the reason that default is now being questioned.
The Terminology Decoded
One of the most confusing things about researching implant placement is the vocabulary. When people say “above the muscle” or “below the muscle,” it sounds like there are only two options. In reality, there are at least four distinct placement planes, and understanding them matters.
Subglandular
The implant sits directly beneath the breast gland and above the chest muscle. There’s no tissue barrier between the implant and the muscle other than natural connective tissue. This is the most straightforward “over the muscle” technique.
Subfascial
The implant is placed under a thin, tough layer of connective tissue called fascia that covers the pectoralis muscle. Think of fascia as a biological sleeve around the muscle. The subfascial position provides additional soft tissue coverage between the implant and the skin compared to subglandular placement. That extra layer helps minimize implant edge visibility and palpability.
Interestingly, a randomized double-blind study found no significant clinical differences between subfascial and subglandular outcomes. The choice often comes down to surgeon experience and patient anatomy.
Prepectoral
This is an umbrella term for any placement above the pectoral muscle. Both subglandular and subfascial qualify as prepectoral. You’ll see this term used interchangeably with “over the muscle” in clinical literature.
Submuscular and Dual Plane
The implant goes partially or fully beneath the pectoralis major muscle. Dual plane is the most common variation: the upper portion of the implant sits under the muscle while the lower portion is covered only by breast tissue. It’s worth noting that dual plane can still cause muscle distortion similar to full submuscular placement, which is one reason patients look into over-the-muscle alternatives.
Quick Comparison Table
Placement | Position | Muscle Cut? | Animation Deformity Risk | Recovery Speed |
|---|---|---|---|---|
Subglandular | Above muscle, below breast tissue | No | None | Fastest |
Subfascial | Above muscle, below fascia | No | None | Fast |
Submuscular | Fully under muscle | Yes | Higher | Slower |
Dual Plane | Partially under muscle | Yes | Moderate | Moderate |
Why Motiva Implants Changed the Over-the-Muscle Conversation
This is the part most articles gloss over, and it’s the most important piece of the puzzle.
Since the early 1990s, the vast majority of breast implants in the United States have been placed under the chest muscle. Surgeons didn’t prefer submuscular placement because it was technically easier (it’s not). They preferred it because the muscle layer helped conceal the edges and normal ripples of older implants. It also reduced capsular contracture rates, which were significantly higher with above-the-muscle placement using traditional implant technology.
So what changed?
Motiva’s SmoothSilk Surface
Motiva’s SmoothSilk surface technology is fundamentally different from the smooth and textured surfaces of traditional implants. Clinical data shows that Motiva’s surface reduces bacterial contamination and biofilm formation, the two primary drivers of capsular contracture. The result: a Baker Grade III/IV capsular contracture rate of just 0.5% at five years.
Critically, the low rates of capsular contracture with Motiva implants are consistent across all surgical planes, whether submuscular, subglandular, or subfascial. That consistency is what reopens the over-the-muscle conversation.
Ergonomix Adaptive Gel
Motiva’s Ergonomix line uses a gel that responds to gravity and body position. When you’re upright, the implant settles into a gentle teardrop shape. When you lie down, the gel redistributes like natural breast tissue. This adaptive behavior produces natural cleavage, a soft upper pole, and a realistic side profile, even when the implant sits above the muscle where there’s less tissue coverage to mask an implant’s shape.
Reduced Rippling
Traditional implants placed above the muscle could cause visible rippling, especially in patients with thinner breast tissue. Motiva’s ProgressiveGel and SmoothSilk surface significantly reduce this risk, removing one of the main reasons surgeons historically avoided prepectoral placement.
The Safety Profile
Beyond capsular contracture, Motiva’s broader safety data is worth noting. Rupture rates are as low as 0.6%. Patient satisfaction sits at 97% at five years. And there have been zero reported cases of BIA-ALCL (breast implant-associated anaplastic large cell lymphoma) linked to Motiva’s smooth implants, compared to 1,380 worldwide cases associated primarily with textured implants from other manufacturers.
The FDA approved Motiva SmoothSilk Round and Ergonomix implants in September 2024 for breast augmentation and revision in women 22 and older. This was the first new breast implant PMA approved by the U.S. FDA since 2013. Since approval, more than 60,000 Motiva implants have been sold in the United States.
For a deeper comparison of how Motiva stacks up against other brands, the differences in surface technology and gel cohesivity are significant. You can explore how Sientra implants and Natrelle implants compare on their respective pages.
Six Benefits of Motiva Over the Muscle
The benefits of placing Motiva breast implants over the muscle fall into six consistent categories that practitioners and clinical data both support.
1. No Animation Deformity
When implants sit under the pectoral muscle, flexing or contracting that muscle can visibly distort the breast shape. This is called animation deformity, and it’s one of the most common complaints with submuscular placement. With over-the-muscle Motiva implants, the pectoral muscle isn’t involved at all, so the breast maintains its shape regardless of movement. This makes the placement particularly appealing for athletes and anyone who regularly does upper body exercise.
2. Faster Recovery
Because the chest muscle isn’t cut or stretched, patients experience less pain and a shorter recovery timeline. The implant sits directly under the breast tissue, creating a natural look with more comfort and significantly less post-operative discomfort. Many patients report returning to normal activities within days rather than weeks.
3. More Stable Long-Term Positioning
With submuscular placement, the pectoral muscle can push on the implant over time, sometimes forcing it too low or too far to the sides. Over-the-muscle placement avoids this dynamic entirely. The implant stays where the surgeon places it, supported by the breast tissue and (in subfascial placement) the fascial layer.
You can learn more about the full breast augmentation recovery timeline for over-the-muscle placement to set realistic expectations.
4. Natural Look and Feel
Motiva’s Ergonomix design mimics natural breast tissue behavior: firmer when standing, softer when lying down. Combined with the breast tissue coverage that over-the-muscle placement provides, the result feels and moves like a natural breast. This is a dramatic improvement over older implants placed in the same position, which often felt firm or looked obviously augmented.
5. Easier Future Revisions
If a patient ever needs a revision breast augmentation or implant exchange, over-the-muscle implants are more accessible. The surgeon doesn’t need to work around or through the pectoral muscle, which means less tissue disruption and a simpler procedure.
6. Shorter Surgical Time
Subglandular and subfascial placement typically involve less dissection than submuscular techniques. Less dissection means less time under anesthesia, less bleeding, and less surgical trauma overall.
Potential Trade-Offs to Consider
No placement option is perfect for every patient. Honest discussion of the trade-offs is important.
Rippling risk in very thin patients. Thin patients with smaller breasts may not be the best candidates for over-the-muscle placement because there’s less tissue covering the implant. While Motiva’s gel and surface technology reduce rippling significantly compared to traditional implants, patients with very little natural breast tissue still face a higher risk of visible implant edges.
Potentially faster aging. Subglandular placement may sag more quickly over time because it follows the natural aging trajectory of the breast tissue without the additional muscular support. For patients concerned about long-term positioning, an internal bra technique can provide supplemental support.
Mammogram interpretation. There are advantages to submuscular placement when it comes to mammogram interpretation. An implant placed above the muscle can overlap with more breast tissue on imaging, potentially requiring additional views. This doesn’t mean mammograms can’t be read accurately with over-the-muscle implants, but it’s worth discussing with both a plastic surgeon and a radiologist.
Limited U.S. data specifically for over-the-muscle. This is a point most articles skip, and it matters. In Motiva’s FDA clinical trial, 94% of participants received implants in a dual-plane pocket. That means the impressive five-year data (0.5% capsular contracture, 97% satisfaction) may not be directly applicable to subglandular or subfascial placement. The international data is encouraging across all planes, but U.S.-specific long-term data for over-the-muscle Motiva placement is still accumulating.
Who Is a Good Candidate?
Candidacy for Motiva breast implants over the muscle depends on anatomy, lifestyle, and goals. Here are the profiles that tend to benefit most.
Women with adequate breast tissue. A simple self-check called the pinch test can give you a rough idea. With your thumb and pointer finger, pinch the skin right above your upper breast pole. If the amount of skin you can grab is 2 centimeters or more, you likely have enough tissue for over-the-muscle placement. This isn’t a definitive test (your surgeon will assess tissue thickness more precisely), but it’s a useful starting point.
Athletes and active women. For those who engage in upper body sports or strength training, avoiding disruption to the chest muscle is a particular advantage. Powerlifters, CrossFit athletes, yoga practitioners, swimmers, and climbers all benefit from keeping their pectoralis major intact.
Revision patients. Women who currently have implants under the muscle and are experiencing animation deformity or muscle-related discomfort may be excellent candidates for switching to over-the-muscle Motiva. An implant exchange in this scenario can solve the animation issue while upgrading to newer implant technology.
Thinner patients (with the right implant). Patients with less natural breast tissue who still want above-the-muscle placement may benefit specifically from the Ergonomix line, whose adaptive gel provides a more forgiving profile under thinner tissue.
If you’re unsure where you fall, a consultation with a plastic surgeon who has experience with Motiva across multiple placement planes is the best next step.
Making the Decision
Choosing between over-the-muscle and under-the-muscle placement isn’t something you should decide based on an article alone. Your anatomy, goals, lifestyle, and the specific implant size and type all factor into the recommendation. Two patients with the same cup size goal might get entirely different placement plans based on their tissue thickness, chest wall shape, and activity level.
What’s changed is that Motiva has made over-the-muscle placement a genuinely strong option for a much wider range of patients. The combination of low capsular contracture rates, reduced rippling, adaptive gel behavior, and zero BIA-ALCL cases means the historical objections to prepectoral placement carry less weight than they used to.
The best way to find out if Motiva breast implants over the muscle are right for you is to discuss your specific anatomy and goals with a plastic surgeon who works with Motiva across all placement planes.
Schedule a consultation with Dr. Leela Mundra to discuss your options for Motiva breast augmentation in Denver.
Frequently Asked Questions
Is over the muscle the same as subglandular?
Not exactly. “Over the muscle” is a general term that includes both subglandular placement (implant directly under breast tissue) and subfascial placement (implant under a thin fascial layer covering the muscle). Both are above the pectoral muscle, but subfascial offers a bit more tissue coverage. Your surgeon will recommend the specific technique based on your anatomy.
Does Motiva over the muscle hurt less than under the muscle?
Yes, consistently. Because the pectoral muscle isn’t cut or stretched, patients report significantly less post-operative pain. The muscle disruption in submuscular placement is the primary source of post-surgical pain, so avoiding it makes a real difference.
Can I get Motiva over the muscle if I have small breasts?
Possibly. Patients with very little natural breast tissue face a slightly higher risk of visible implant edges, even with Motiva’s improved gel and surface. However, the Ergonomix line’s adaptive behavior helps compensate. The pinch test (grabbing at least 2cm of tissue above the upper breast pole) gives a rough indication of candidacy. A surgeon’s hands-on assessment during a consultation is the definitive answer.
Will my mammograms be affected by over-the-muscle placement?
Implants above the muscle can overlap with more breast tissue on mammographic imaging, sometimes requiring additional views. This doesn’t make mammograms unreliable, but it’s worth mentioning to your radiologist and discussing with your surgeon beforehand. Submuscular placement does offer a slight advantage in mammogram interpretation.
How long do Motiva implants last?
Motiva’s five-year data shows a rupture rate as low as 0.6% and a reoperation rate of 6% for primary augmentation patients. No breast implant is a lifetime device, and most surgeons recommend monitoring over time. But Motiva’s durability profile is strong compared to previous implant generations.
What is animation deformity and does over-the-muscle prevent it?
Animation deformity happens when the pectoral muscle contracts (during exercise, lifting, or even just flexing) and visibly distorts the shape of an implant placed beneath it. It ranges from subtle shifting to dramatic movement. Over-the-muscle placement eliminates this entirely because the implant has no contact with the pectoral muscle.
How do I know if over the muscle or under the muscle is right for me?
The honest answer: you won’t know until a qualified surgeon evaluates your tissue thickness, chest wall anatomy, breast shape, implant size goals, and activity level. Motiva has made over-the-muscle placement viable for far more patients, but under-the-muscle is still the better choice for some. A thorough consultation is the only way to make this decision well.